

.
|
Noviembre, 2000
Guillem Feixas i Viaplana
Luis Ángel Saúl Gutiérrez
Several personal construct researchers have focussed their interests on the construction of symptoms. Fransella (1970) suggests, for example, that the symptoms can become a way of life for the client and a part of his/her identity. The alternative to presenting such symptoms might imply the relative absence of predictions about one's self. In the same vein, in this discussion of the resistance to change of anorexic clients, Button (1983) considers that such patients may tend to preserve their thinness because they do not have alternative dimensions available through which to anticipate themselves, both in themselves and in their relation to others. Also Winter (1982), has found that the constructions which clients make about their symptoms can maintain a highly consistent logic given that they represent strongly held beliefs.
A interesting starting point in the study of these conflicts was developed by Hinkle (1965) who focused on the clinical meaning of these dilemmas. In these studies, we observe in some situations patients symptom construction are associated with positive implications which are often related to characteristics which define the client's own identity. The abandonment of such symptoms would represent a threat for the self. In these situations the patient faces a dilemma in which he/she wishes to abandon the symptoms, with all their negative effects and yet, this symptomatology has positive connotations and implications for the self. Its abandonment would involve the patient shifting to an opposed, unclear and undesirable pole (see also Catina, 1990; and Tschudi, 1977). In Winter's (1982) more typical dilemma study, for example, it appears that many depressed subjects associate their symptoms with sensitivity and other virtues. Many people with agoraphobic symptoms associate being independent with a high possibility of being unfaithful. Subjects that consider themselves timid appear to associate being socially skilled with a wide variety of negative characteristics (selfish, vain, insensitive, arrogant, inconsiderate, etc.). Ryle (1979) shows three ways of constructing the symptom which he calls dilemmas, traps and snags. Catina's (1990) outcome study shows that the way in which clients construe their symptom is of clinical relevance.
Some authors, for example Ryle (1979), argue that the success of brief dynamic therapy depends on adequate patient motivation, high therapeutic involvement and activity, and the clear identification of a focus for treatment. A purpose of our research project is to concentrate on the latter and determine ways in which the focus of brief therapy could be conceptualised more precisely. We believe that research focussed on dilemma detection and resolution (the therapeutic work's focus) could shed new light on the clarification of the 'resistance' to symptom change, and to the understanding of success in therapy.
A CONSTRUCTIVIST PERSPECTIVE
In spite of the fact that the client may be experiencing a certain amount of problems or suffering, the constructivist perspective believes that the stance which a person takes with regard to their life is coherent with their vision of themselves. The notion of dilemma which we present, based on the choice corollary (Kelly, 1955), assumes that a person chooses those alternatives from her own construct poles which are more meaningful and coherent with her construct system, i.e. those retaining the greater predictive power. To keep her world predictable, a person tries to protect her identity from invalidation, structured as a network of nuclear constructs. This constructivist view is in contrast with an hedonistic one (see Winter, 1985) suggesting that people organise their behaviour in order to search for pleasure and avoid suffering. If we take this latter view, how should we explain the presence of discrepant constructs in which the subject prefers one pole but instead of simply moving to the desired pole he/she continues at the same pole with some degree of suffering (Botella & Feixas, 1998; Mancini, 1992). By taking the constructivist stance mentioned above, we assume at the outset that the person is making a "wise" choice in terms of her personal coherence. This view contrasts with other more traditional views that label the client's processes with terms such as "distorted thoughts", "cognitive errors", "irrational beliefs", "dysfunctional learning processes", or others which attribute the problem to unconscious motives and conflicts. So the issue then becomes; why the desired change in the discrepant construct does not occur? In which sense this change, if occurring, would make the subject's world less predictable? Which aspects of her sense of coherence or of her sense of identity, would become invalidated? Which of the subject's construct poles are being validated by acting in a way that includes symptoms and suffering?. The idea is that by simply pushing for a shift to the desired pole of the discrepant construct we can trigger on the client a series of actions (traditionally labelled as "resistance") oriented to preserve her sense of identity, and thus the predictive power of her construct system. By detecting implicative dilemmas we intend to reveal the coherence of the client's actions according to their construct system. We hypothesise that working in therapy respecting this coherence will enhance the therapy alliance and preclude opposing actions (or "resistance"); this resulting in a better therapeutic outcome.
PREDICTED EFFECTS OF IMPLICATIVE DILEMMAS ON THERAPEUTIC OUTCOME
Were considered the construction of the symptom is an important issue for the reconstruction process during therapy. Because of the implications of these dilemmas, the patient feels him/herself divided between a desirable change and the symptom’s positive relation with the patient's self-definition. Catina, et al. (1990) found that the more positive implications the patient's symptomatic behaviour presented, the more difficult it was for him/her to reach his/her desired goals, whereas reduction of positive symptom implications led to a better treatment outcome.
Therapeutic success has been found to be positively related to the decrease of implicative dilemmas, for different therapy approaches (Winter, 1991). It is not clear, however the inverse, resolving dilemmas reduces the symptoms. If this inverse relationship were to be established it would be of enormous advantage, at least for cognitive and some brief psychodynamic therapies, due to the viability to detect foci (i.e. dilemmas) to work on from even the first sessions.
THE UTILITY OF THE DETECTING OF IMPLICATIVE DILEMMAS
In summary, we consider two important contributions in the detection and work with implicative dilemmas:
a) Understanding the symptom as a coherent option for the person
Unlike notions such as ‘resistance’ and ‘cognitive distortion’ found in other approaches, the focus on implicative dilemmas is advantageous because it understands the client’s in the context of coherence. Likewise, from the constructivist epistemology, the client's position of 'no change' is presented as a process of self-protection which shelters the coherence, the systemic integrity, and protects the client from a sudden 'nuclear' change (Feixas & Villegas, 1991).
This leads us towards a co-constructive psychotherapeutic endeavour which takes coherence into account such a fashion that the client can find a flexible space in his/her construct system which allows him/her elaborate an alternative construction.
The focus on the client’s construct system is in keeping with Kelly's goal of the 'acceptance of the client' (1955), a definition which leads the therapist to use the patient's own construct systems. According to Kelly (1955), the therapist ought to try and use the patient's vocabulary and meaning system.
Reframing the problem in terms of a dilemma involving the client’s sense of coherence and identity has the effect of making the client feel accepted, thereby reducing his or her anxiety. This allows him/her to begin to consider alternative constructs (Feixas & Villegas, 1991), a process which Kelly (1955) termed circumspection.
b) The focus of the therapy process
Focussing on the dilemma leads to a reframing of the patient's problem. This reframing has to be shared with the patient in terms which are acceptable to him/her. Using the same terms that the patient uses to make sense of his/her world, helps to not distance this interpretation from his/her frame of reference.
For the patient, this reframing involves seeing what he/she has communicated in a new way. By focusing on the dilemma, it is hoped that the patient will find a coherence and useful explanation of his/her suffering, both of which should facilitate symptom reduction across time.
The neurotic difficulties, and in particular the lack of agency or self-efficacy which are part of many patients' experience, are related to the terms by which he/she constructs his/her world. Those terms can be conceptualised as 'implicative dilemmas'. As long as the client can only see the possibility of actions within the terms of his/her dilemma, change will be unlikely. The degree to which these terms are known to the patient, or the degree to which he/she can be aware of them, varies. The first task for the therapist is to extend those understandings; once the implicative dilemmas are understandable by the patient, they can become an appropriate focus for therapy.
FUTURE DIRECTIONS
We believe that the study about clients’ constructions of their symptomatology can help us to understand better their system coherence with respect to non-change whilst helping to establish negotiated strategies with them in order to work on an alternative construction in which the dilemma does not appear. At the same time, we believe that a dilemma focussed approach provides us with both a focus for therapy and a frame which attributes coherence to the client’s suffering.
Although we see this type of approach as useful and promising, we believe that more detailed research is needed into the implications of dilemma focussed work with clients and its relationship with the disappearance of the given symptomatology.
METHODOLOGY: Client Assessment Procedures |
CODES:
Each case is assigned a code. This is composted for 4 figures:
| 1 | 2 | 3 | 4 | |||||
| CODE: |
1: It is the code for the place. Salamanca is 1, Barcelona 2, London 3, etc.
2: It is the year
3: It is the code for the therapist
4: It is the case number for that therapist
TEST BATTERY AND ASSESSMENT POINTS
The following tests will be used:
As a general orientation, the format would include 12 sessions, beginning weekly and then using a two-week interval when appropriate. Three assessment points during the therapy, and two at follow-up, are suggested. Particularly, assessment at point 2 is optional.

Fig. 1. Flow chart illustrating measures administered at each of the five assessment points.
Usually, during the first session, the intake, the client’s demand/complain is elaborated. All the assessment questionnaires will be filled in by the client after the therapy session. If there is not a room where the clients can stay for filling them in, the test forms could be given to them to take home and collected in the next session.
At the end of the first session the SCL-90R and the BDI questionnaires will be given to the client. Within the two first sessions the therapist will carry out a clinical assessment taking in account the CIE 10 or DSM-IV criteria. According with this assessment it will be applied a specific symptomatic instrument either to be completed by the client or by the therapist, as in the Hamilton inventory in the case of depression. If the presence of a personality disorder has not been ruled out with the clinical interview –that is, the clinician suspects criteria for personality disorder could be applied-- it will be also given the MCMI-II questionnaire at the end of the second session. The RGT will be administered during the second session.
The same initial test battery will be used for the following assessments, except for the MCMI-II questionnaire if it was used.
Optionally, questionnaires for the second assessment will be given at the end of the seventh session and collected in the next one.
For the end-of-therapy assessment they will be given at the end of the eleventh session.
To carry out the two follow-up assessments the questionnaires can be sent by post with a return envelope in case a follow-up session is not feasible. These follow-up assessments will be at three and twelve months after the end of the therapy.
As a twelve-session is the standard format, some therapy processes may need a longer or shorter time period. The number of sessions can be recorded as a variable to be controlled for some analysis.
The Repertory Grid Technique (RGT)
Following Sue Watson’s dissertation (1998), the grid format to be used consists of 15 elements and 15 constructs. The elements are Self Now, Self Before Problems Began, Self in 6 Months, Mother, Father, Partner, Child or Sibling, My therapist, Two Significant People, a Man and a Woman I Like, a Man and Woman I Dislike and Ideal Self (a model to be used can be found as an appendix). This list is a general proposal and could be adapted to specific client situations (e.g., no siblings or children, or more than one which is significant) even to the point of slightly modifying the number of elements.
The RGT will be completed as follows. At the first assessment (second session), the researcher explained to the client that the two of them are going to carry out an exercise which would help the researcher to understand how the client views his or her world. The researcher, then, produces fifteen cards on which the element role titles are written, whilst says to the client "I’m going to give you some descriptions of people that might be in your life. I want you to think of a person who fits that description and give me a first name for them". Each element card will be placed in front of the client until he or she have thought of an appropriate person and supplied a name, which the researcher wrote on the card.
The researcher could usually trigger a response by explaining that the person need not to be currently in the client’s life, but may be a figure from the past, for example someone from a previous workplace. Clients who have not previously encountered a Therapist will be asked to imagine what sort of a person a Therapist would be, and to evoke this fantasy figure when requested. If an imaginary Therapist is used, then this element will not be used for the elicitation of constructs, but only during the subsequent rating of the elements on the constructs. If the client discloses that a particular person, e.g. Mother or Father have been absent, the researcher will ask for the name of the person who have most closely fulfilled that role for the client. If the social network of a client is so constricted instead of choosing personal acquaintances, media or historical figures could be used in his/her grid.
Once the elements have been identified, the researcher will use the triadic method to elicit 13 constructs from the client. A group of three elements including the Self Now will be placed in front of the client, who will be then asked to consider and then tell the researcher "some important way in which two of these people are alike, but different from the third person". When the client has thought of a similarity between two of the elements, for example ‘selfish’, this is recorded as the emergent pole of the construct. The client is then asked to describe someone who is the opposite of ‘selfish’, thereby eliciting the implicit, or contrast pole. This procedure is repeated with different elements, including the Self Now in every triad to ensure self-relevant constructs, until 13 constructs are elicited. The other self elements are not used in the elicitation procedure.
If the therapist finds it easier for the client to use the dyadic method it can be used. In this case the Self Now should be used with the most relevant constructs. A selection of relevant dyads to be presented are: father-mother, self-father, self-mother, self-sibling, self-partner.
To obtain constructs 14 and 15, the client is asked to tell the researcher "two problems or difficulties that you feel that you have which may be why you have decided to seek therapy". Having disclosed two problems, the client is then asked to provide a contrast pole for each problem construct. In the case the client had already elicited problem-constructs before arriving to construct 14, and no other problems can be identified, two other constructs are included.
When all 15 constructs have been elicited, the client is then invited to rate each element on each construct, using a 7 point rating scale.
The same set of constructs and elements will be used for further grid assessments.
|
COMPONENTS OF AN IMPLICATIVE DILEMMA
(Feixas, Saúl & Sánchez, 1999)

STEPS to identify Implicative Dilemmas:
1. IDENTIFY THE CONGRUENT AND DISCREPANT CONSTRUCTS.
Table 1. Criteria used to identify Congruent and Discrepant Constructs in a seven point scale grid (Feixas & Sánchez, 1998).
- Congruent Constructs: difference between Self and Ideal-Self Ł 1
- Discrepant Constructs: difference between Self and Ideal-Self ł 4
2. STUDY THE CORRELATIONS BETWEEN THE CONGRUENT AND DISCREPANT CONSTRUCTS.
Table 2. Correlation scores to establish the presence of a Implicative Dilemma (Feixas & Sánchez, 1998)
|
INTERVENTION ON IMPLICATIVE DILEMMAS |

REFRAMING THE PROBLEM IN TERMS OF A DILEMMA |
Redefinition of the patient's problem as a dilemma between the desire for change and the difficulty to do that, producing a "blockage" and a respectable suffering in the client. It is presented how this "blockage" has a coherence and a internal logic.
The client’s problem is reframed as a dilemma between the desire for change and the difficulty to do that. This conflict paralyses the client’s development with considerable suffering and symptomos.
To do the reformulation the following aspects are taken into account:
DILEMMA ELABORATION |
GOALS:
SPECIFIC WORK WITH THE CONSTRUCTS INVOLVED IN THE DILEMMA
TYPE OF ELABORATION |
TYPE OF CONSTRUCTS |
POSSIBLE TECHNIQUES |
| Ascending implication of each constructs |
|
Ascending laddering |
| Descending implications of each constructs |
|
Downward laddering |
| Tacit rules of implication |
|
Downward Arrow |
| Symptom coherence |
|
Tschudi's ABC |
WORKING THROUGH THE DILEMMA'S IMPLICATIONS |
ASCENDING LADDERING
ORIGIN:
The ascending laddering technique was proposed by Hinkle (1965, doctoral dissertation directed by Kelly). This technique is part of the implication grid proposed by this author.
GOAL:
The laddering process serves as an exercise of clarification of value which helps the client make sense of underdeveloped self-aspects.
TECHNIQUE APPLICATION:
| 1. | Take the discrepant construct of the dilemma. |
| 2. | Ask the client which of the two poles of the construct describes better the type of person he or she prefers to be. |
| 3. | Asks the client why he/she prefers to be "X" instead of "Y". This can be done also in terms of which are the advantages of "X" and the disadvantages of "Y" just as he/she sees it. |
| 4. | The procedure is repeated upon this new construct and the subsequent until the client can not elicit more superordinate dimensions (or is beginning to repeat him/herself). |
Although this procedure is well structured as described above, it should be conducted in a conversational mode rather than a list of questions.
DOWNWARD LADDERING OR PYRAMIDING (Landfield, 1971)
ORIGIN:
It is a variant of the laddering technique. The pyramiding technique was proposed by Landfield (1971) based on the Individually Corollary (Kelly, 1955).
GOALS:
TECHNIQUE APPLICATION:
The same process is repeated with the "discrepant construct/s" which are involved in the dilemma.
DOWNWARD ARROW
ORIGIN
This technique was proposed by some cognitive therapists (for example, Burns, 1980) with the purpose of eliciting the chain of inferences which lead the client to a given conclusion from a specific fact. However, apart from this use, Neimeyer (1993) proposed also to evaluate the tacit implication rules which lead the connection between "evidence" and "conclusion".
GOALS:
TECHNIQUE APPLICATION:
|
The questioning and the redefinition of each of the connections can be a therapeutic end in itself.
TSCHUDI'S ABC (Tschudi, 1977)
GOALS:
TECHNIQUE APPLICATION:
The goal of this technique is to elicit three related constructs:
The continuation of the therapy adopts the way of trying to generate and explore alternatives which allow the client to conserve the positive implications of the constructs B and C simultaneously.
Example:
A |
|
|
B |
|
|
C |
|
|
CONTROLLED ELABORATION |
Suggested by Kelly (1955), it can be defined as hte attempt to make consistent and communicable one part of the client's construct system to make it possible to contrast its validity.
GOALS:
PHASES:
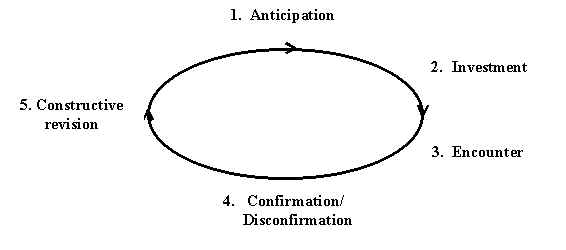
Experience Cycle
RECONSTRUING IMMEDIATE EXPERIENCE OF THE DILEMMA |
ORIGIN OF THE TECHNIQUE (Guidano, 1991)
During this phase we utilise the "Moviola technique" presented by Guidano (1991) to lead client's observation of his/her worrying present vital experiences related with the dilemma.
GOALS:
TECHNIQUE APPLICATION
ANALYSING THE RELATIONSHIP TRAP |
Relevant figures of the client’s interpersonal world may play an important role in the maintenance of the dilemma. In these case the client is immersed in what Ryle (1979) calls "relational traps". This aspect should be explored, and relational traps, if found, can be identified and elaborated.
GOALS:
PROCEEDURE:
HISTORICAL RECONSTRUCTION OF THE DILEMMA |
ORIGIN:
The deepest origins of the "historic reconstruction" can be found in psychoanalysis, but we were influenced more by other authors such as Kelly, Mahoney, Guidano, and Gonçalves. We found the Gonçalves' method the more elaborated (Gonçalves, 1993; 1994a; 1994b; 1995a; 1995b; 1995c; 1995d; 1995e, 1997a, 1997b).
GOALS:
The historic reconstruction can be made even after the end of the process.
NARRATIVE ELABORATION |
This section is focussed on the work with client's writings, without taking into consideration the larger concept of narrative.
Therefore, we can focus on sessions in some client's self-biography writing or we can create tasks asking the client for writings giving dilemmas' examples, alternatives, or being critic with it, etc.
GOALS:
SOME TASKS:
ROLE PLAYING THE DILEMMA |
One of the optional phases we propose in the dilemma elaboration work is the elaboration of those dilemmas through dramatisation techniques, depending on the client's symbolic and imaginative capacity and the abstraction level we achieved in the dilemma elaboration.
GOALS:
DIFFERENT TASKS:
The client spatially represents the dilemma. He/she uses the therapy room to place each dilemma pole (congruent, undesirable, present and desired). In the same way he/she materialises the impediments for his or her change and places them also in the room. For this the client can use chairs or other objects to represent those barriers. The client passes physically between poles and from each one manifests his sensations, emotions, dubs, fears, etc. The therapist helps the client to elaborate of this material with his/her questions.
It is a typical technique of the Gestalt Therapy, which we propose for the client's experiential work with each of the dilemma terms.
The principal goal of this intervention is to help through the dialogue between the two poles of the discrepant construct to a integrative solution (Greenberg, et al., 1993).
SOLUTION ELABORATION |
EXCEPTIONS TO THE DILEMMA
Following Steve de Shazer (De Shazer y cols., 1986; De Shazer, 1991) we define the dilemma's exceptions as those occasions in which, against all odds, the dilemma is not given.
Characteristics:
TECHNIQUE STEPS:
- Elicit the exception
- "Mark" the exception
- Expand
- To attribute control
- To go on
Therapist: In which moments lately have you felt less depressed and at the same time less worried about the others
Client: Yesterday, I was helping my brother. I felt very much at ease there. I felt well
Therapist: Is that so? And in the times when you were helping your brother, how are you feeling?
SCALING QUESTIONS |
They are largely used in family therapy.
They are an important resource to generate information, establish goals, identify advances and attribute responsibility for the changes.
GOALS:
FORMULATION OF THE SCALE:
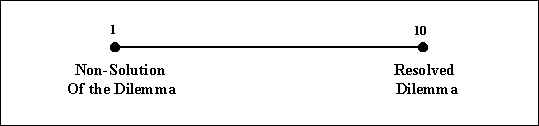
"In a scale from 1 to 10, in which 1 is the moment in which the dilemma has been worst and 10 is the moment in which it will be solved, in which point you placed the last week?
POSSIBLE SCALES TO WORK WITH THE DILEMMA:
Dilemma Scale:
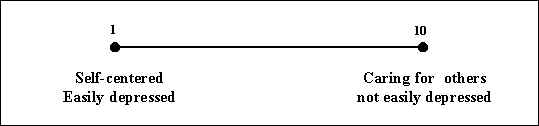
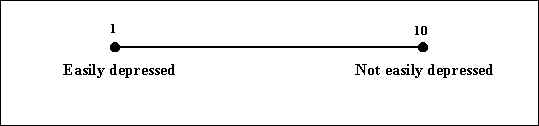
Symptom Scale:
Confidence Scale:
"On a scale of 1-10, in which 10 will mean you have all the confidence in the world to maintain this level and 1 will mean you do not have any confidence at all, where do you place yourself?"
THE MIRACLE QUESTION |
ORIGIN:
The techniques of future projection are new in psychotherapy, the origin goes back to the use of the hypnosis.
In the field of brief therapy, De Shazer described in 1972 an Ericksonian resource with the name of "crystal ball technique". It consists in asking the client (in a trance state) to imagine a future without the problem. In recent years, De Shazer has developed a variant of this technique, the "Miracle question" (De Shazer, 1988, 1991).
Through this technique total protection is given to the client from the imagination world, as Kelly pointed: "this is probably the oldest protective screen that man uses to go into the unknown" (Kelly, 1955; pg. 373).
FORMULATION
GENERATION OF ALTERNATIVES |
Through the preceding phases different alternatives are been generated to live without the dilemma, in this moment we can to summarise them and generate even more absurd ones.
GOALS:
PROCEDURE:
We can work with all theses alternatives in imagination, role playing or making possible real contacts to check them.
REFLECTING ON THE CHANGE PROCESS |
The work presented in this phase has to do with helping the client will realise that the change exists and is possible. In this phase we attempt to help the client verify his/her own change process, awarding him/her the control which he/she deserves and presenting the process as a learning and maturation one.
Equally the client is becoming aware that life is full of difficulties, but in that also is the richness and variety of life, being the process of learning from experience the most enriching process of the person's life.
GOALS:
PROCEDURE:
FIXED ROLE OF THE RESOLVED DILEMMA |
A optional phase in the dilemma resolution work is the work from the presentation of a "fixed role of the solved dilemma". It is an adaptation of Kelly's technique (1955). The client is asked to represent a role, designed by the therapist, in which apart form others characteristics, the congruent and desired poles of the dilemma are present. So in this role the dilemma is not present.
GOALS:
REFERENCES |
Burns, D. (1980). Feeling good. Nueva York: Signet.
De Shazer, S. (1986). Claves para la solución en terapias breves. Buenos Aires: Paidós.
De Shazer, S. (1988). Clues. Investigating solutions in brief therapy. New York: Norton.
De Shazer, S. (1991). Putting difference to work. New York: Norton.
Feixas, G., & Sánchez, V. (1998). Orientación para el análisis de rejillas. Unpublished manuscript.
Gonçalves, O. F. (1995d). Psicoterapia cognitivo-narrativa. Revista De Psicoterapia, 7, 101-112.
Guidano, V. F. (1991). The self in process. New York: Guilford.
Kelly, G. A. (1955). The psychology of personal constructs (Vols. I, II). New York: Norton.
Neimeyer, G. J. (1993). Constructivist Assessment: A casebook. Londres: Sage Publications.
Tschudi, F. (1995). FLEXIGRID Manual. Oslo: University of Oslo.
APPENDICES |






TSCHUDI’S ABC
1 |
2 |
3 |
4 |
|||||
| CODE: |
Date:..........................
A |
(Present Pole) | (Desired Pole) |
B |
(Disadvantages) | (Advantages) |
C |
(Advantages) | (Disadvantages)
|
![]() Home
Home
![]()