TC

-
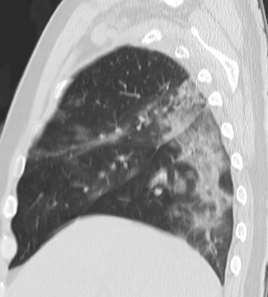
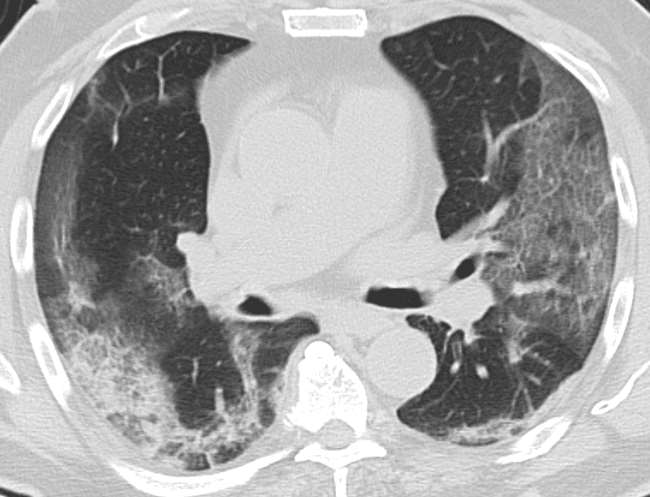
Ground-glass opacity
-
Multiple lobes
-
Subpleural or peripheral distribution (center is usually preserved)
-
Septal thickening
-
Bronchial thickening
-
Pulmonary consolidations / “crazy paving” pattern (advanced di)
-
Predominantly peripheral, basal and generally bilateral
-
No nodules, no pleural effusion, no cavitation
- Ground-glass opacity and peripheral distribution (subpleural)

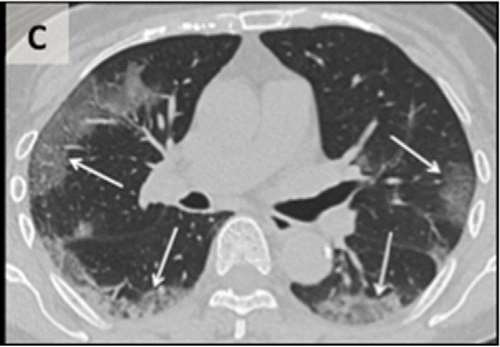
Ground-glass opacity is a descriptive term referring to an area of increased attenuation in the lung with preserved bronchial and vascular markings.
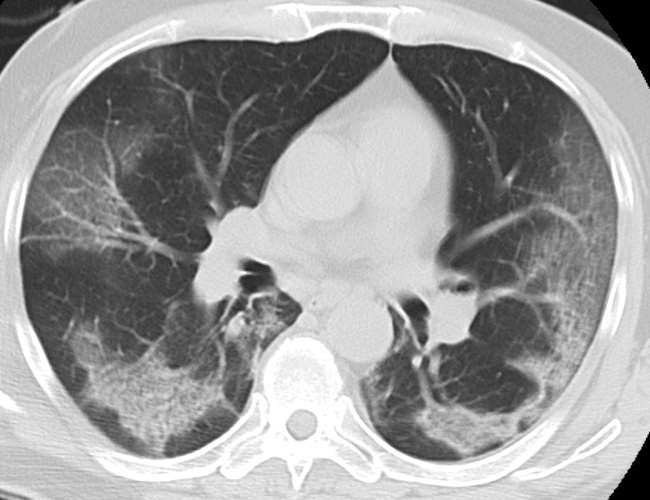

-
Multiple lobes

- Septal and bronchial thickening


- Crazy paving
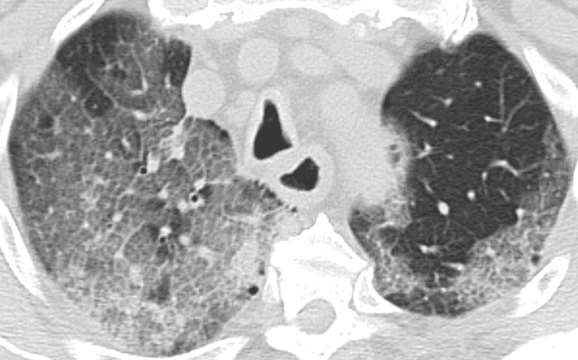
The “crazy-paving” pattern is a common finding at thin-section computed tomography (CT) of the lungs. It consists of scattered or diffuse ground-glass opacity with superimposed interlobular septal thickening and intralobular lines that give the illusion of polyhedral shapes that resemble paving stones.
Clinical case 1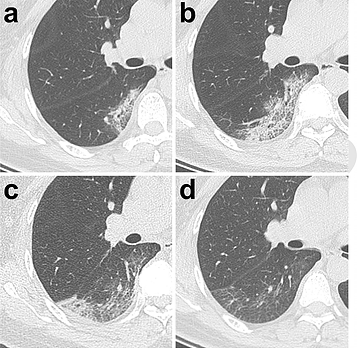

47-year-old-woman with 3-day-long-fever (38,8ºC)
- Day 3: ground-glass opacities located in a small subpleural region and partial consolidation in the inferior right lobe.
- Day 7: the region where ground-glass opacities were located expands. Septal thickening (both interlobular and intralobular, also known as "crazy-paving") appears. Partial consolidation is also present.
-
Day 11: ground-glass opacity pattern partially resolves. A new area of subpleural consolidation appears.
-
Day 20: ground-glass opacity pattern resolution continues. Prenchymal lines are present.
Clinical case 2
77-year-old male
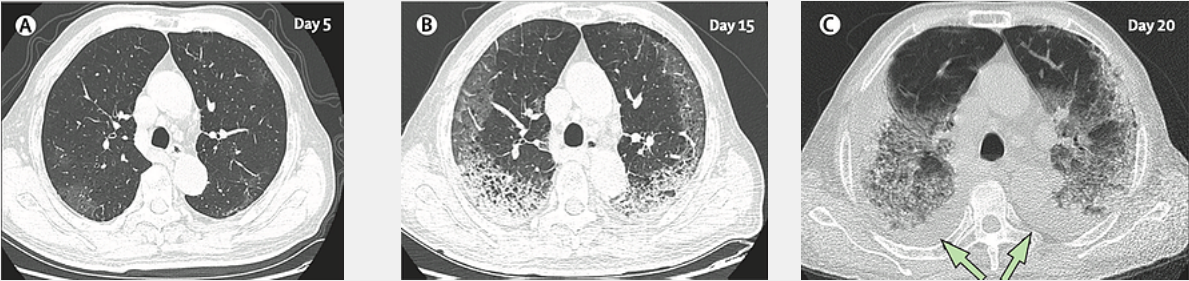
- Day 5 after symptom onset.
Patchy ground-glass opacities affecting the bilateral, subpleural lung parenchyma.
-
Day 15 after symptom onset.
Subpleural crescent-shaped ground-glass opacities in both lungs, as well as posterior reticular opacities and subpleural crescend-shaped consolidations. -
Day 20 after symptom onset.
Expansion of bilateral pulmonary lesions, with enlargement and denser pulmonary consolidations and bilateral pleural effusions (arrows). The patient died 10 days after the final scan. The patient died 10 days after this CT.
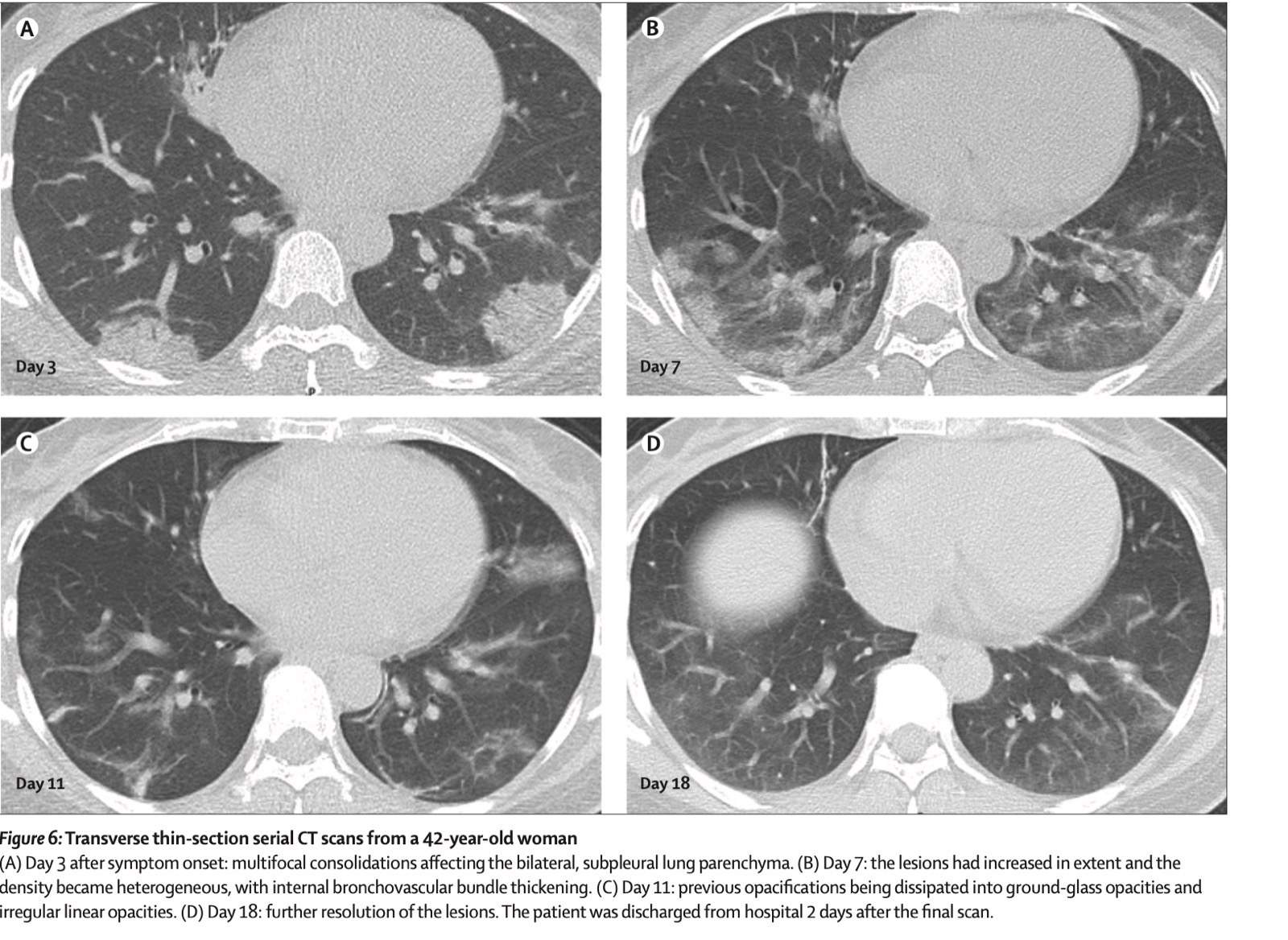
Clinical case 3
42-year-old female
- Day 3 after symptom onset: multifocal consolidations affecting the bilateral, subpleural lung parenchyma.
- Day 7: the lesions had increased in extent, and the density became heterogeneous, with internal bronchovascular bundle thickening.
-
Day 11: previous opacifications being dissipated into ground-glass opacities and irregular linear opacities.
-
Day 18: further resolution of the lesions. The patient was discharged from hospital 2 days after the final scan.
-
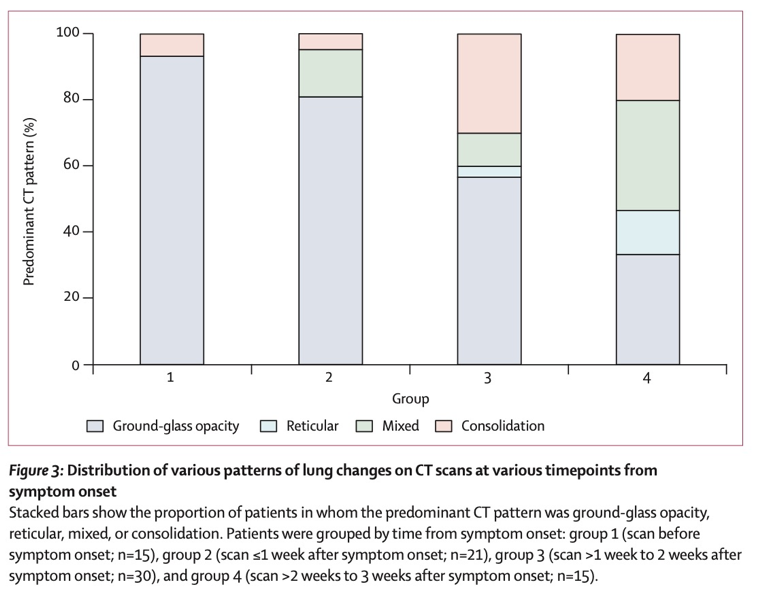
In the asymptomatic stage, the most common finding is ground-glass opacity (present in 90% of patients).
-
During the first week the findings remain the same. However, in some cases signs of consolidation appear.
-
During the second week, after the symptom onset, the number of cases with ground-glass opacities decrease whereas sign of consolidation or the coexistence of both patterns (ground-glass opacity + consolidation) increase.
-
During the third week, most patients present a mixed pattern.